
প্রথমেই জেনে নিচ্ছি এর মানে কি?
৩টা ভাগে পড়লে আমাদের বুঝতে সুবিধা হবে তাই সেভাবেই লিখছি:
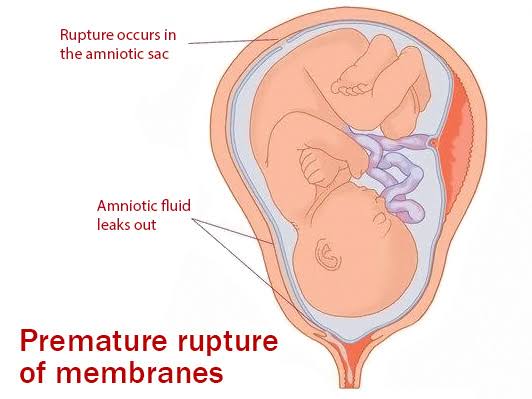
▪︎ Spontaneous rupture of the membranes
▪︎ Any time beyond 28th week of pregnancy
▪︎ But before onset of labour is called premature rupture of the membrane (PROM).
তাহলে প্রশ্ন আসে membrane rupture সাধারণত কখন হয়?
উত্তর- After full dilatation of cervix in 1st stage of labour.
আমরা 37 weeks এর উপর depend করে একটা baby কে term & preterm বলে থাকি।
So,
Types of PROM:
1. Preterm PROM : Membrane ruptures before 37 completed weeks.
2. Term PROM: Membrane ruptures beyond 37th week before labour starts.
কেন এই PROM হচ্ছে? Risk factor গুলো নিয়ে আলোচনা করলে আমরা পাচ্ছিঃ
1. Preconceptional cause:
▪︎ Repeated genito-urinary infection
▪︎ Cervical incompetence
▪︎ Chronic cervicitis
▪︎ Obesity
▪︎ Smoking
▪︎ Low socioeconomic status
▪︎ Nutritional deficiency
2. Pregnancy related :
▪︎ Polyhydramnios
▪︎ Multiple gestation
▪︎ Abortion
▪︎ Fetal abnormalities
▪︎ Previous history of PROM
3. Genital tract infection (with):
▪︎ Group B streptococcus
▪︎ Bacterial vaginosis
▪︎ Candida
▪︎ Mycoplasma
▪︎ Ureaplasma hominis
▪︎ E.coli
▪︎ Staphylococcus
How to diagnose?
যখন একটা patient PROM নিয়ে আসবে সে আমাদের কাছে বলবে তার watery discharge হচ্ছে per vaginally. So, যখন clinical features এর কথা বলব তখন,
Symptom : Sudden gush of fluid per vagina.
Sign:
🌸 Per-abdominal examination:
Fluid loss এর কারণে height of the uterus will be reduced than the period of gestation.
🌸 Sterile gentle speculum examination:
To inspect the liquor & odour escaping through the cervix.
🌸 To examine the collected fluid from posterior fornix:
👉 For Nitrazin test/ Litmus paper test:
কেন করব?
কারণ, during pregnancy normal vaginal pH is 4.5-5.5, যেখানে liquor amnii এর pH হচ্ছে 7-7.5.
Litmus paper এর রঙ যখন yellow থেকে blue হবে তখনই বোঝা যাবে যে there is presence of liquor amnii.
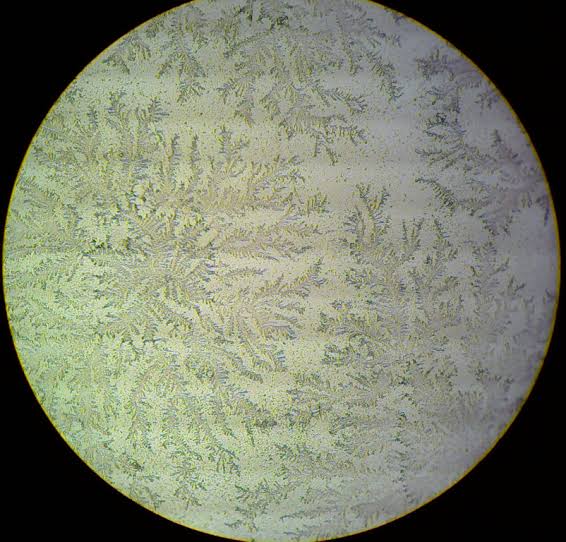
👉 For Fern test:
Visualization of ‘fern-pattern’ on a slide under low-power on a microscope.
👉 For Nile Blue Sulphate (0.1%) test:
To see the presence of exfoliated fat cells from sebaceous glands of foetus.
🌸 যেহেতু discharge আছে সেহেতু আমরা oligohydramnion এর features পেতে পারি।
মা হয়ত বলবে বাচ্চার movement কম পাচ্ছে,
palpation করলে আমরা uterine contraction পেতে পারি।
🌸 যদি দেখি যে Patient has raised temperature তখন ভাবতে হবে chorioamnionitis নিয়ে।
Chorioamnionitis এ আমরা কয়েকটা জিনিস বিবেচনা করব।
👉 Prolonged PROM (>24hrs)
👉 Raised temperature
👉 Severe lower abdominal pain
👉 Foul smelling P/V discharge
আর এই ক্ষেত্রে investigation করলে
👉 Leukocytosis
👉 Increased C-reactive protein (CRP) পাব
👉 এরপর আমাদের high vaginal swab নিতে হবে for culture
👉 Ultrasonography ও করতে হবে।
Investigations:
1. Complete blood count –
(Chorioamnionitis হলে leukocytosis পেতে পারি)
2. C-reactive protein (CRP) –
(Chorioamnionitis এ raised থাকে)
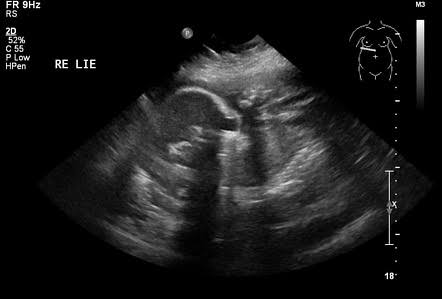
3. Ultrasonography –
(To detect:
Gestational age, Biophysical profile,
50- 70% of woman with PROM have low amniotic fluid,
Rule out other cause)
4. Endocervical swab for gram stain and culture
(To exclude genital tract infection)
5. Fetal fibronectin assay
(If foetal fibronectin is present in cervical secretion it indicates preterm birth, usually found between 22-34 weeks; in PROM sensitivity: 98.2%)
6. Amnisure
(Detects PAMG-1/placental immunoglobulin; it is a protein produced by decidual part of placenta & found in amniotic fluid after rupture of membrane.
99% sensitivity, 100% specificity)
7. Urine R/M/E
8. CTG
9. Nitrazin test
10. Fern test
11. Nile blue sulphate test
Treatment of PROM:
1. General Treatment :
▪︎ Hospitalization
▪︎ Bed rest with bathroom privilege
▪︎ Wearing of clean vulval pad
▪︎ Counselling of mother
▪︎ Maternal & fetal monitoring
2. Specific Management of PROM:
a) Expectant management –
(যদি preterm PROM, no evidence of chorioamnionitis থাকে)
🌸 Expectant management এ আমরা যা করব:
👉 Antibiotics: Ceftriaxone 1gm BD for 3 days.
👉 Corticosteroid: Oradexon 6gm 12hrs apart
👉 Tocolytics ( 48 hours to allow lung maturity)
b) Active management –
♣ যদি term PROM, chorioamnionitis, fetal distress, fetal anomalies থাকে)
👉 Active management মানে হল termination of pregnancy.
♣ Preterm PROM without chorioamnionitis হলে আমরা যেভাবে treatment করব:
🌸 Gestational age <24weeks:
👉 Active termination due to poor prognosis.
🌸 Gestational age 24-34 weeks:
👉 Expectant management
👉 Delivery at 34 week
🌸Gestational age >34 weeks but <37 weeks:
👉 Expectant management
👉 Active management :
▪︎ Induction of labour with oxytocin
▪︎ LUCS (যদি কোন obstetric indication থাকে তাহলে)
♣ Term PROM without chorioamnionitis :
👉 Cervix ripe না হলে expectant management করতে হবে & wait for 6-12 hours to allow ripening & spontaneous onset of labour.
👉 Cervix ripening হলে active management করতে হবে।
▪︎ Induction of labour with oxytocin
▪︎ LUCS (যদি কোন obstetric indication থাকে তাহলে)
PROM with chorioamnionitis :
👉 Termination of pregnancy irrespective of gestational age.
Mode of termination :
🌸 যদি cervix favourable হয়, fetal condition ভালো থাকে তাহলে induction of labour with oxytocin and vaginal delivery করব।
🌸 যদি vaginal delivery contraindicated হয় তাহলে caesarean section করতে হবে।
Complications :
A. Maternal complications :
▪︎ Chorioamnionitis
▪︎ Placental abruption
▪︎ Dry labour
▪︎ Sepsis
B. Fetal complications :
▪︎ Fetal pulmonary hypoplasia
▪︎ Respiratory Distress Syndrome,intraventricular haemorrhage, necrotizing enterocolitis
▪︎ Fetal distress due to cord compression
▪︎ Increased perinatal morbidity
Faria Mehrin
JRRMC
Session: 2014-15
প্ল্যাটফর্ম একাডেমিয়া/ ফাহিমা হাসান