
General Surgery এর একটা অত্যন্ত গুরুত্বপূর্ণ টপিক হচ্ছে ‘Shock’।
★ আসেন প্রথমে আমরা জানি – “What is shock?”
Shock may be defined as systemic state of low tissue perfusion that is inadequate for normal cellular respiration.
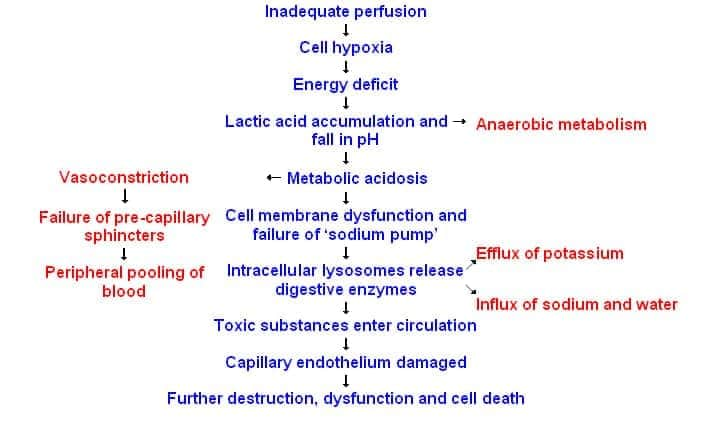
★ এখন আমরা আসি – “What is the pathophysiology of shock?”
আমরা জানি যে, যেহেতু tissue perfusion কমে যাচ্ছে, তার মানে cell-এ oxygen-ও কমে গেছে। আর cellular respiration (i.e. aerobic metabolism) এর জন্য দায়ী oxygen। So, oxygen কম মানে, there will be shift of aerobic to anaerobic respiration. And the end product is lactic acid (so lactic acidosis).
Secondly, Cell এর যে energy-র উৎস oxygen, শেষ হয়ে যাবে এবং Cell membrane এবং intracellular organelle এ যে energy depedent sodium-potassium pump থাকে, তা আর কাজ করতে পারবে না। যার ফলে intracellular lysosome থেকে enzyme release হবে এবং cell lysis হবে। যার ফলে potassium ও রিলিজ হবে blood এ।
Lastly, এই hypoxia, যার ফলে acidosis, সব মিলায়ে complement cascade, free radical activation & ultimately endothelial damage করে ফেলে। Which is responsible for activation of coagulation system and leakage of fluid to interstitial spaces leading to tissue oedema.
তাছাড়াও multiple system এ specific effect আছে shock এর।
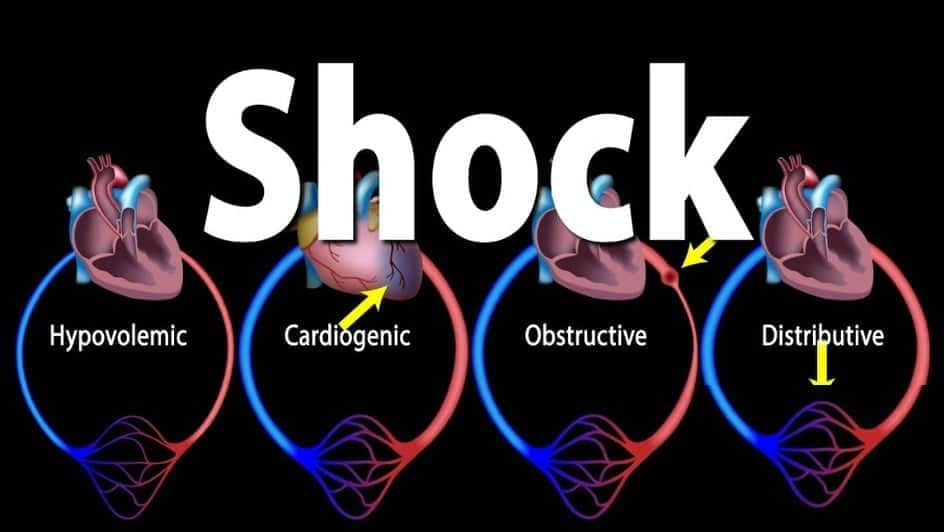
★ Now, “What are the types of shock?”
- Hypovolemic shock,
- Cardiogenic shock,
- Obstructive shock,
- Distributive shock,
- Endocrine shock.
এই সব shock এ কি হচ্ছে, না হচ্ছে, তা আমাদের সবারই কম-বেশি জানা আছে, তাই আর বিস্তারিত বললাম না। I will just focus on some important points.
★ So, “What is Distributive shock?”
আমরা আগে pathology তে septic shock কে shock এর classification হিসেবে পড়ে এসেছি। কিন্তু এইখানে মজার ব্যাপার হচ্ছে septic shock is a type of distributive shock।
So, Distributive shock comprises of 3 types of shock. That is –
- Septic shock,
- Anaphylactic shock and
- shock following Spinal cord injury.
In all these cases, there is loss of vascular tone, vasodilatation and peripheral pooling of the blood.
★ Now, What is Endocrine shock?
এই টার্ম টাও অনেকটা নতুন।
So, this is nothing but the combination of hypovolaemic, cardiogenic or distributive shock. But, it may also occur independently/ alone in some endocrine disorder like (Hypo/ Hyperthyroidism)
★ Now there is an interesting factor, আমরা এই যে এত সময়ে different types of shock দেখলাম, “How Can we clinically differentiate?”
এর আগে আমরা জানি one of the important parameter of shock সম্পর্কে – that is ‘𝐁𝐚𝐬𝐞 𝐝𝐞𝐟𝐢𝐜𝐢𝐭’।
Base deficit – জিনিসটা হচ্ছে, deficient level of base needed to titrate blood pH towards normal.
So, It will be High in all kinds of shock (I repeat, all kind of shock). So, দেখাই যাচ্ছে parameter-টা কত গুরত্বপূর্ণ।
Base deficit কেন high পাব আমরা। ব্যাপারটা আরও সহজ। আমরা pathophysiology-তে দেখেছি, anaerobic respiration এর ফলে lactic acid তৈরি হচ্ছে। এখন এই অনেক পরিমাণ lactic acid কে neutralize করার জন্য যে পরিমাণ base (মানে bicarbonate) লাগবে, তার ঘাটতি রয়েছে (i.e. DEFICIT)। So, obviously it will be High.
Now, lets come to the interesting point, একটা parameter আমরা জানলাম। Now, “there is a difference between distributive (septic) shock and all other shocks.” আমরা জানি, সব ধরনের shock এ cardiac output কমে এবং vascular resistance বাড়ে।
But, in Septic shock, ঠিক উল্টা। আমরা জানি, there is loss of vascular tone causing vasodilation and peripheral pooling of blood here. So, বুঝাই যাচ্ছে cardiac output বাড়বে, তার মানে peripheral resistance-ও কমবে (But, lately আমরা typical feature of shock পেতে পারি)।
আমরা clinically septic shock এ warm periphery & capillary refill time rapid পাব (ঐ একই কারণ vasodilation etc) but বাকি সব shock এ cold, clammy periphery and proloned capillary refill time।
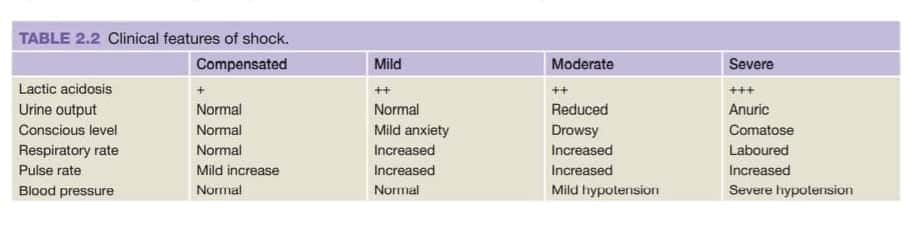
★ “What is the severity of shock?”
এই জিনিসটা বুঝার জন্য, একটা clear conception দরকার, তাহলেই আমরা severity কে আলাদা করতে পারবো।
আচ্ছা, একটা মানুষের blood pressure আর urine output normal-এর উপর নির্ভর করে কি বলে দিবেন patient shock এ নাই?
– কখনোই না। এই patient mild shock এ থাকতে পারে (occult hypoperfusion এর কারণে সব vitals and urine output normal)।
তাহলে প্রশ্ন জাগে, আমরা confirm হবো কিভাবে? (আগেই যে বলেছিলাম, Base deficit সব ধরনের shock এ বাড়ে – এখন বুঝা গেল এর গুরুত্ব। সাথে serum lactate-ও বাড়বে)।
এই occult hypoperfusion ১২ ঘন্টার বেশি যদি persist করে, তাহলে Multiple organ failure হয়ে death ও হয়ে যেতে পারে। বুঝাই যাচ্ছে কতটুকু dangerous- এক কথায় silent killer।
★ Severity সম্পর্কে জানলাম। এখন আসি একটা shock এর patient কে কিভাবে resuscitate করব।
Airway, Breathing control করেই আমাদের উদ্দেশ্য থাকবে যত দ্রুত সম্ভব Fluid resuscitation। কারণ আমদের hypoperfusion prevent করাই মূখ্য উদ্দেশ্য।
আমরা যদি patient এর cause of shock সম্পর্কে না জানি , তখন কি করব? Bailey & Love এ এই ব্যপারে সুন্দর একটি ব্যাখ্যা আছে:
“𝐈𝐟 𝐭𝐡𝐞𝐫𝐞 𝐢𝐬 𝐢𝐧𝐢𝐭𝐢𝐚𝐥 𝐝𝐨𝐮𝐛𝐭 𝐚𝐛𝐨𝐮𝐭 𝐭𝐡𝐞 𝐜𝐚𝐮𝐬𝐞 𝐨𝐟 𝐬𝐡𝐨𝐜𝐤, 𝐢𝐭 𝐢𝐬 𝐬𝐚𝐟𝐞𝐫 𝐭𝐨 𝐚𝐬𝐬𝐮𝐦𝐞 𝐭𝐡𝐞 𝐜𝐚𝐮𝐬𝐞 𝐢𝐬 𝐡𝐲𝐩𝐨𝐯𝐨𝐥𝐚𝐞𝐦𝐢𝐚 𝐚𝐧𝐝 𝐛𝐞𝐠𝐢𝐧 𝐰𝐢𝐭𝐡 𝐟𝐥𝐮𝐢𝐝 𝐫𝐞𝐬𝐮𝐬𝐜𝐢𝐭𝐚𝐭𝐢𝐨𝐧, 𝐚𝐧𝐝 𝐭𝐡𝐞𝐧 𝐚𝐬𝐬𝐞𝐬𝐬 𝐭𝐡𝐞 𝐫𝐞𝐬𝐩𝐨𝐧𝐬𝐞.”
এখন suppose একটা patient এর bleeding হচ্ছে। আপনি কি শুধু fluid দিয়েই resuscitate করে যাবেন? অবশ্যই না- তার তো already ongoing fluid loss হচ্ছে, তার উপর আপনি দিচ্ছেন আরও fluid, ত লাভটা কই হইল। Fluid loss তো চলছেই।
তাহলে এই case এ আমরা কি করব?
সহজ হিসাব- আপনার উত্তর হবে “I will identify the bleeding site and control the haemorrhage with side by side simultaneous resuscitation.”
অন্যদিকে, একটা patient এর bowel obstruction এর কারণে hypovolaemic shock-এ আছে, সেই patient এর surgery লাগবে। তখন obviously preoperative fluid resuscitation করে surgery তে পাঠাইতে হবে, অন্যথায় আরও hypovolaemia exacerbate হবে এবং organ failure-ও হতে পারে।
(এই প্রসঙ্গে একটা জিনিস বলে ফেলি- bowel obstruction এ যে hypovolaemia হচ্ছে, তার কারণটা কি? এইখানে 3rd space fluid loss হয়। এখানে 3rd space বলতে বুঝাচ্ছে interstitial space of GIT। Bowel obstruction ছাড়াও pancreatitis-এ 3rd space loss হয়)
★ 𝐒𝐡𝐨𝐜𝐤 এর 𝐩𝐚𝐭𝐢𝐞𝐧𝐭 কে আমরা কি 𝐟𝐥𝐮𝐢𝐝 দিব, আর কতটুকু দিব?
এ নিয়ে অনেক debate আছে। তবে প্রকৃতপক্ষে there is no difference in response or outcome between crystalloid or colloid solution.
এই ক্ষেত্রেও কথা আছে – usually sodium containing fluid (Normal saline) দেয়া হয় না কারণ বেশি হয়ে গেলে it may cause hyperchloremic metabolic acidosis। So, buffer solution (Hartmann’s/ Ringer’s lactate solution) is preferred.
But, ‘নাই মামার চেয়ে তো কানা মামাই ভাল’- শুধু normal saline তখন available থাকলে normal saline দিয়েই resuscitate করতে হবে।
আরেকটা জিনিস হচ্ছে: Resuscitative fluid হিসাবে কখনো 5% DA দেয়া যাবে না (body’র বাইরে 5% DA Isotonic, body তে ঢুকার পরে, glucose metabolize হয়ে, hypotonic হয়ে যায়। আর hypotonic-এর কাজ জানি আমরা- ফ্লুইড cell-এ ঢুকে যায়, intravascular volume আর expand হইল না। সুতরাং হইল হীতে বিপরীত – তাই ভুলেও দেয়া যাবে না)।
So, আমরা বলতে পারি “𝐒𝐮𝐜𝐜𝐞𝐬𝐬𝐟𝐮𝐥 𝐢𝐧𝐢𝐭𝐢𝐚𝐥 𝐫𝐞𝐬𝐮𝐬𝐜𝐢𝐭𝐚𝐭𝐢𝐨𝐧 𝐝𝐞𝐩𝐞𝐧𝐝𝐬 𝐦𝐨𝐫𝐞 𝐨𝐧 𝐭𝐡𝐞 𝐫𝐚𝐩𝐢𝐝𝐢𝐭𝐲 𝐚𝐧𝐝 𝐚𝐝𝐞𝐪𝐮𝐚𝐜𝐲 𝐨𝐟 𝐟𝐥𝐮𝐢𝐝 𝐫𝐞𝐩𝐥𝐚𝐜𝐞𝐦𝐞𝐧𝐭 𝐭𝐡𝐚𝐧 𝐨𝐧 𝐭𝐡𝐞 𝐜𝐡𝐨𝐢𝐜𝐞 𝐨𝐟 𝐫𝐞𝐠𝐢𝐦𝐞𝐧.”
★ এখন আসি কতটুকু 𝐟𝐥𝐮𝐢𝐝 দিব?
Bailey and Love-এ স্পষ্ট লেখা আছে, 250-500 mL fluid আমরা ৫-১০ মিনিটের মধ্যে দিয়ে দিব (তবে খেয়াল রাখতে হবে, যাতে volume overload না হয়ে যায়, আর নাইলে hypothermia , dilutional coagulopathy হয়ে patient মারা যাবে)।
Patient response এর উপর ভিত্তি করে আবার patient কে ৩ ভাগে ভাগ করা হইল (Responder, Transient responder and Non-responder) যার বিস্তারিত আলোচনায় আর না-ই গেলাম।
★ 𝐇𝐨𝐰 𝐰𝐢𝐥𝐥 𝐲𝐨𝐮 𝐦𝐨𝐧𝐢𝐭𝐨𝐫 𝐚 𝐩𝐚𝐭𝐢𝐞𝐧𝐭 𝐢𝐧 𝐬𝐡𝐨𝐜𝐤?
A) Minimum:-
- ECG,
- Pulse oximetry,
- Blood pressure (Permissive hypotension- Systolic blood pressure 70-90 mmHg পর্যন্ত),
- Urine output (Target urine output is > 0.5 ml/kg/hour).
B) Additional:-
- Central venous pressure,
- Invasive blood pressure,
- Cardiac output,
- Base deficit and Serum lactate.
★ 𝐖𝐡𝐚𝐭 𝐢𝐬 𝐭𝐡𝐞 𝐞𝐧𝐝 𝐩𝐨𝐢𝐧𝐭 𝐨𝐟 𝐫𝐞𝐬𝐮𝐬𝐜𝐢𝐭𝐚𝐭𝐢𝐨𝐧? (কত সময় ধরে 𝐟𝐥𝐮𝐢𝐝 দিব?)
আমরা vital parameters (BP, Pulse & urine output) এর উপর নির্ভর করে থাকবো না। আগেই বলেছিলাম, occult hypoperfusion এ এই সব normal। So, we should rely on the global perfusion end points (Base deficit, serum lactate).

ধৈর্য্য ধরে পড়ার জন্য ধন্যবাদ। চেষ্টা করেছি, যত টুকু জানি, সহজ ভাষায় জানানোর।
Reference-
Bailey and Love 27th edition (chapter-2)
Principle and practice of surgery (APM Forrest)
Rafid Aziz Chowdhury,
Session:- 2015-2016,
Jalalabad Ragib Rabeya Medical college, Sylhet.
Platform academic / Ariful Islam Neloy