

It is a degenerative disease of the synovial joint characterized by focal loss of articular hyaline cartilage with proliferation of new bone and remodeling of bone contour.
(Disease of articular cartilage not bones)
➡ Commonly affects the weight-bearing joints such as the knee and hip joint.
➡ Affects woman more. (post menopausal as there is loss of estrogen)
➡ Genetic predisposition is the key factor in osteoarthritis (OA)

Pathophysiology of Osteoarthritis:
Degeneration of articular cartilage is defining feature of osteoarthritis
⬇
Normally chondrocyte are terminally differentiated cell, but in osteoarthritis
⬇
Chondrocyte differentiate further and produce nest of metabolically active cell➡ first, matrix components are produced at increased rate but in the same time major structural components of matrix are degraded (aggrecan and type II collagen)
⬇
loss of aggrecan concentration in the matrix causes the cartilage to become vulnerable to load bearing injury
⬇
Fissuring of cartilage surface➡ develop deep vertical cleft
⬇
localised chondrocyte death and cartilage thickness is reduced
⬇
Large cartilage damage and calcium pyrophosphate and calcium phosphate deposit in the abnormal cartilage
▶ Clinical feature:
➡ Pain on weight bearing activity and movement but the pain relief on rest.
➡ Early morning stiffness usually less than 15 minutes.
➡ Restricted joint movement.
➡ Swelling around joint (knee joint).
➡ Jerky gait (knee joint involvement).
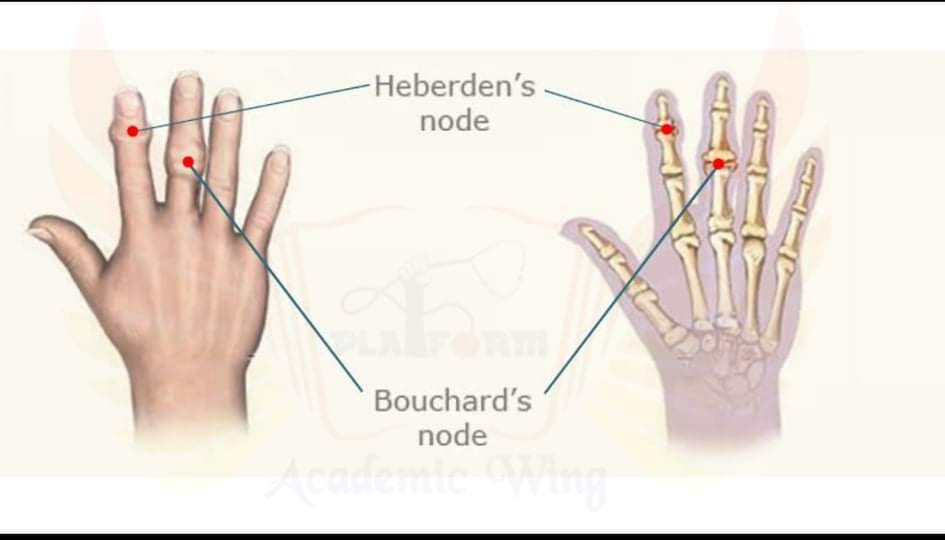
➡ Patient may present with nodules in the hand (Distal interphalangeal joint & proximal interphalangeal joint) in generalized nodal OA.
➡ Patient may complain of crackling sound of the joint of walking or weight lifting, which is also heart of physical examination.

▶ Hand Nodules are usually found in later stages of OA (H/o of Knee OA+)
Heberden’s nodule- found in distal interphalangeal joint.
Bouchard’s nodule- found in Proximal interphalangeal joint.
▶ Increase calcium pyrophosphate deposition in the Knee joint can lead to pseudo-gout formation in the knee joint.
▶ Investigation:
- Plain Xray
- Synovial fluid aspiration
- Rheumatoid factor
▶ What will you find in and Xray that’s suggestive of Osteoarthritis?
➡ Narrowing of joint space
➡ Osteophytes
➡ Subchondral cysts
➡ Subchondral osteosclerosis
➡ Joint deformity.
▶ Management:
➡ Weight loss in obese patients
➡ NSAID
➡ Intra-articular glucocorticoids
➡ Muscle strengthening exercises.
Sushmita Chowdhury
USTC/IAHS
2015-2016
platform academia/ Tohfa Rahman Galib