
Chronic Kidney Disease
(দ্বিতীয় পর্ব)
Causes আর pathophysiology জানার পর এবার ধাপে ধাপে শিখি কিভাবে CKD এর patient কে evaluate করা যায়।
প্রথমেই আগে থেকে কোন Co-morbidities আছে কিনা অথবা drug এর history আছে কিনা জেনে নিব like
- Known CKD
- DM
- HTN
- Drugs (e.g. NSAIDS, Lithium, Cyclosporin, ACEi, ARB etc)
- Congestive cardiac failure
- Atherosclerotic diseases
- Multisystem disease with possible renal involvement (e.g SLE, Myeloma)
- Urologically unexplained haematuria
- Family history of kidney disease
এই History গুলো কোন patient এর থাকলে CKD এর screening করতে হবে।
CKD এর Investigation জানার আগে এই screening কিভাবে করা যায় জেনে নেই।
- Urine analysis for blood and protein(+/- PCR if possible)
- Blood Pressure
- eGFR
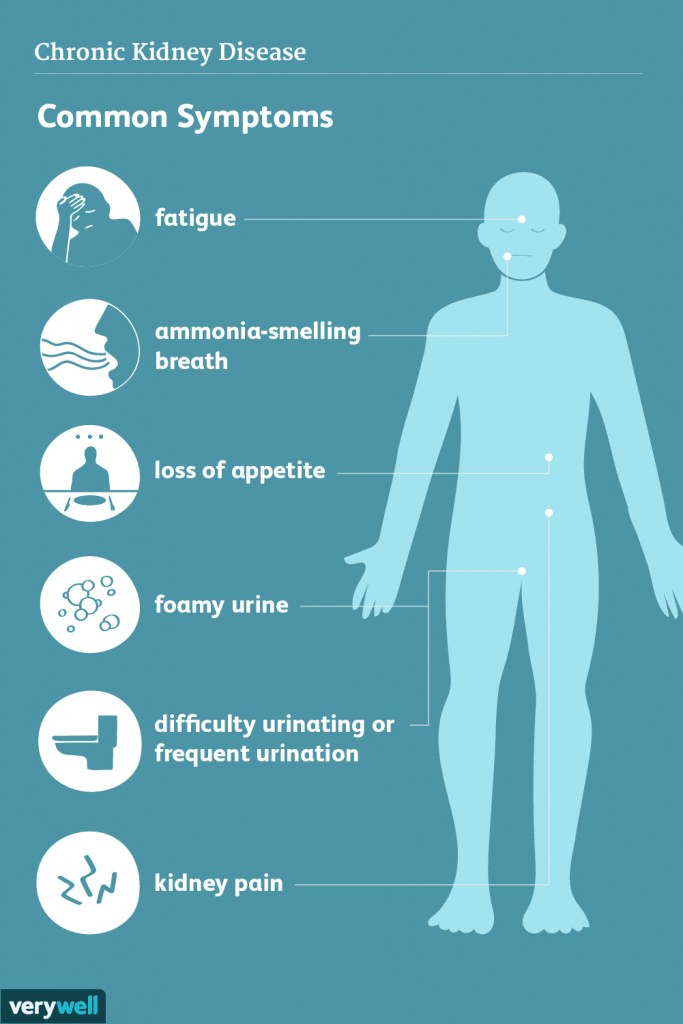
এবার আসি Patient কী কী sign symptoms নিয়ে appear করতে পারে :-
Symptoms গুলো প্রথমে দেখি
- patient may remain asymptomatic (untill GFR falls below 30ml/ min)
- Nocturia maybe the initial symptom
- Hiccups
- Anorexia
- Weight loss
- Tiredness & breathlessness
- Nausea, diarrhoea or vomiting
- Insomnia
- Parasethesia, itching (Due to excretory problem)
- Symptoms of anaemia (Due to impared erythropoietin function)
- Bone pain
- In case of female there may be amenorrhea and in case of male erectile dysfunction (due to adrenal insufficiency)
-Mental slowing, clouding of consciousness, myoclonic twitching and seizure may found in advanced uraemia
এই symptoms গুলো নিয়ে patient আসতে পারে।
এরপর যে Sign গুলো দেখবো:-
- Anaemia
- HTN
- Increased respiratory rate / Kussmaul breathing (Due to profound metabolic acidosis)
-Yellow brown complexion (due to concentration of urea) - Raised JVP
- Brown line pigmentation of nails
- Bruising
- Excoriation of pruritus
- Pericardial friction rub
- Absent reflexes, parasethesia, reduced sensation may develop as a result of peripheral neuropathy
এই sign symptoms গুলো মোটামুটি সব CKD patients দের থাকে।
International guideline অনুযায়ী CKD কে GFR count আর clinical presentation এর উপর কয়েকটি stage এ ভাগ করা হয়:-
Stage 1: Kidney damage with normal or increased GFR (>90 mL/min/1.73 m2)
Stage 2: Mild reduction in GFR (60-89 mL/min/1.73 m2)
Stage 3A: Moderate reduction in GFR (45-59 mL/min/1.73 m2)
Stage 3B: Moderate reduction in GFR (30-44 mL/min/1.73 m2)
Stage 4: Severe reduction in GFR (15-29 mL/min/1.73 m2)
Stage 5: Kidney failure (GFR < 15 mL/min/1.73 m2 or dialysis)
Stage 1, 2 এবং 3A তে mild to moderate CKD বলা হয়। এসময় sign symptoms তেমন দেখা যায় না।
Stage 3B থেকে sign symptoms appear করে এবং আস্তে আস্তে severity-এর দিকে যায়।
Stage 5 এ kidney failure হয়। এসময় replacement করা না হলে death might occur।
এবার আসি কী কী criteria থাকলে patient কে অবশ্যই nephrologist এর কাছে reffer করবো :-
• eGFR < 30 mL/ min/ 1.73 m2
• Rapid deterioration in renal function (> 25% from previous or > 15 mL/ min/ 1.73 m2/ year)
• Significant proteinuria (PCR > 100 mg/ mmol or ACR > 70 mg/
mmol) , unless known to be due to diabetes and patient is already on appropriate medications
• ACR > 30 mg/ mmol with non-visible haematuria
• Hypertension that remains poorly controlled despite at least four antihypertensive medications
• Suspicion of renal involvement in multisystem disease
এগুলোর মধ্যে যেকোনো একটা থাকলেও nephrologist এর কাছে reffer করতে হবে।
এবার আসি কী কী investigation করতে হয় এবং কেনো করতে হয় জেনে নেই।
- Urea and creatinine:- To assess stability/ progression compare to previous results.
- Urinalysis and quantification of proteinuria:-
Haematuria and proteinuria may indicate glomerular disease and need for biopsy. - Proteinuria:- It indicates risk of progressive CKD requiring preventive ACE inhibitor or ARB therapy.
- Electrolytes:- To identify hyperkalaemia and acidosis.
- Calcium, phosphate, parathyroid hormone and
25(OH)D are done for the assessment of renal osteodystrophy. - Albumin:- Low albumin consider malnutrition, inflammation, nephrotic syndrome.
- Full blood count (±Fe, ferritin, folate, B12) :- If anaemic, we should exclude common non-renal explanations, then manage as renal anaemia.
- Plasma lipids, blood glucose ± HbA1c, ECG is given for cardiovascular patients who have high risk in CKD.
- Renal ultrasound:- Only if there are obstructive urinary symptoms, persistent haematuria, family history of polycystic kidney disease or progressive CKD. Here small kidneys suggest chronicity and asymmetric renal size suggests renovascular or developmental disease
- Hepatitis and HIV serology:- If dialysis or transplant is planned. Hepatitis B vaccination recommended if seronegative.
- Some other tests can also be given according to clinical background.
ভেবে দেখলাম রানু চাচীর যে Investigation reports গুলো দেখেছিলাম ওখানে উনার GFR ছিলো 18 mL/min/1.73 m2। উনার Anaemia, HTN, severe weight loss, anorexia, increased respiration, peripheral neuropathy সহ আরো কিছু sign symptoms একদম prominent ছিলো।
এজন্যই তাঁর stage 4 CKD patient হিসেবে treatment চলছে।
পরবর্তী ধাপে treatment আর complications নিয়ে বিস্তারিত জানার চেষ্টা করবো।
(to be continued)
Reference :-
Davidson’s Principle & Practice of Medicine (23rd edition)
Kumar & Clarke’s Clinical Medicine ( 8th edition and 10th edition)
Platform academia/ Fariha Bintay Amin (Nodi)
Institutions of Applied Health Science, Chittagong.
Session:- 2015 – 16
Pingback: Important Discussion About Chronic Kidney Disease(Part -3) – Platform | CME