
Fasting in Ramadan is obligatory for all healthy Muslim adults. No food or drink can be consumed between sunrise and sundown. Among the benefits of fasting apart from heeding the Creator’s order is to teach self-restraint and discipline as well as resting and cleansing the alimentary tract. The call to fast during Ramadan for a healthy Muslim is stated in the holy Quran, where there is also a clear guide on individuals who are exempted from fasting which includes those with diseases that may endanger their life (Surah Al Baqarah Verse 184-185).
Many Muslims around the world wish to fast during Ramadan due to religious reasons, though some of them suffer from chronic diseases like Diabetes and Hypertension. It is the responsibility of the medical professionals to empower Diabetic patients to make an informed choice and if possible, an evidence-based decision regarding safe fasting in Ramadan.
MEDICAL BENEFITS OF FASTING :
• Decrease in body weight.
• Increase in high-density lipoprotein (HDL) cholesterol with or without any changes in total cholesterol and triglycerides levels.
• Improvement in glycemic control in diabetics.
• Decrease in daytime average systolic and diastolic blood pressures in hypertensive patients.
• Improvement in immunity by elimination of toxins, reducing insulin-like growth factor 1 (IGF-1) which allows the regeneration of stem cells in bone marrow.
• Reduce cardiovascular disease markers such as C-reactive protein (CRP) and plasminogen activator inhibitor type-1 (PAI-1).
RISKS ASSOCIATED WITH FASTING :
• Hypoglycaemia
• Hyperglycemia with crisis e.g. DKA/HONC
• Dehydration
• Thrombosis
DIABETIC PATIENTS WHO CANNOT FAST DURING RAMADAN :
• Severe hypoglycemia/DKA/HONC within last 3 months prior to Ramadan
• Patient with H/O recurrent hypoglycaemia
• Patient with hypoglycemic unawareness
• Patient with sustained poor glycemic control
• Type 1 DM on multiple insulin injections per day (3 or more)
• Acute illness : Overt cardiovascular disease e.g. Recent MI, hepatic dysfunction
• Pregnancy with poor glycemic control
• Patients on chronic dialysis
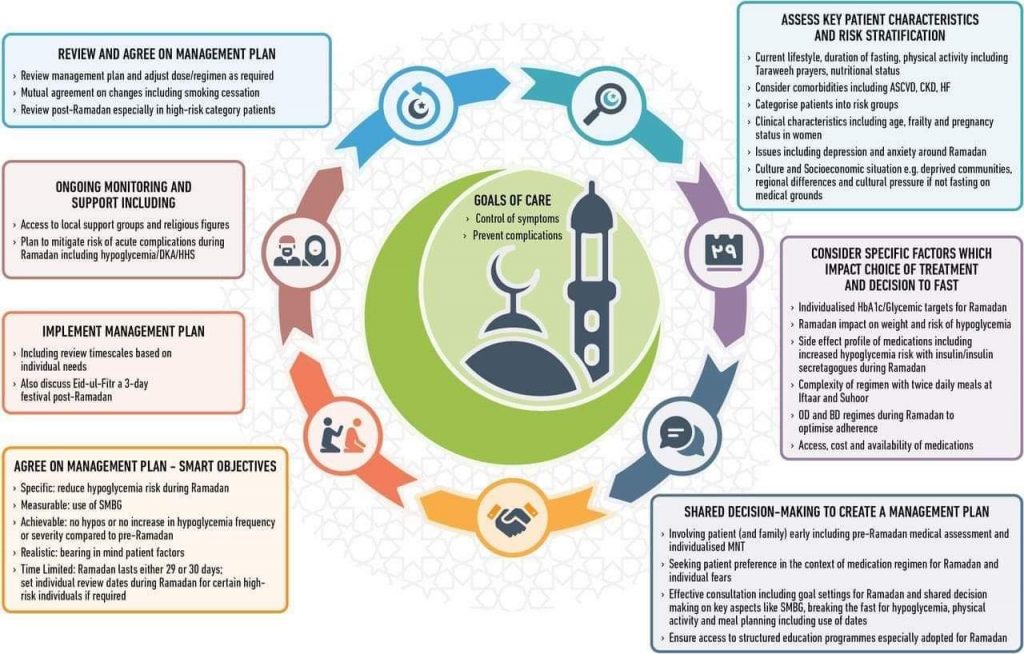
INDIVIDUALIZATION OF DIABETES MANAGEMENT DURING RAMADAN :
• Care must be individualized.
• Management plan will differ for each specific patient.
EDUCATION AND COUNSELLING OF DIABETIC PATIENTS ABOUT RAMADAN :
Education of diabetic patients and their families regarding –
• Acute complications and their management and how to prevent them
• Blood sugar monitoring
• Meal planning
• Physical activity
• Drug and dose adjustment
DIET PLAN :
• Never skip sahur (dawn meal). Sahur should consist of balanced meal with adequate carbohydrate taken as late as possible to avoid unnecessary prolonged fasting.
• Do not delay Iftar. Limit intake of high-sugary foods. However, 1-2 dates at start of iftar according to Sunnah may be taken as part of carbohydrate exchange.
• Supper after Tarawih can be taken as replacement of pre-bed snack.
• Include fruits and vegetables at both sahur and iftar. Limit fried or fatty foods.
• Sufficient fluid must be taken to replenish fluid loss during the day. Choose sugar-free drinks. Drink adequately at sahur.
EXERCISE :
. • Avoid rigorous exercise during fasting time because of risk of hypoglycemia.
. • The timing of exercise is preferably 1-2 hours after the break of fast.
. • Performance of Tarawih night prayers helps to maintain physical activity.
ORAL ANTI-DIABETIC DRUG MODIFICATION DURING RAMADAN :
• Metformin : Daily dose remains unchanged. Immediate release preparation taken once daily should be taken at Iftar, for twice daily dose, should be taken at Iftar and suhoor and for thrice daily dose, morning dose should be taken at suhoor with combine afternoon and evening dose at iftar. Prolonged release preparation should be taken at iftar.
• Sulfonylurea : Switch to newer Sulfonylurea (Gliclazide, Glimepiride) where possible and Glibenclamide should be avoided. For once daily dose, should be taken at Iftar. Dose may be reduced in patients with good glycemic control. For twice daily dose, dose remains unchanged but Suhoor dose may be reduced in patients with good glycemic control.
• Meglitinides : Thrice daily dosing may be reduced/redistributed to two doses taken with iftar and suhoor.
• Acarbose : No dose modification.
• Thiazolidinediones : No dose modification, can be taken at Iftar or suhoor.
• Dipeptidyl peptidase-4 Inhibitors : No dose modification.
• SGLT2 inhibitors : No dose modification. Dose should be taken with iftar. Extra clear fluids should be ingested during non-fasting periods. Should not be used in the elderly, patients with renal impairment, hypotensive individuals or those taking diuretics.
INSULIN MODIFICATION DURING RAMADAN :
. • Premixed insulin regimen : Usual morning dose at iftar and half of the usual evening dose at sahur
. • Split mixed insulin regimen : Usual morning dose of regular insulin and NPH at iftar and half of the usual evening dose of regular insulin and NPH at sahur
. • Basal bolus insulin regimen : Usual morning and lunch dose of rapid acting analogs at iftar and night meal and 50% of dinner dose at sahur and half of long acting analog at fixed time
. • GLP-1 analogue : Same dose preferably at iftar

BLOOD GLUCOSE MONITORING :
• Blood glucose level during fasting : To recognize subclinical hypo or hyperglycemia
• 2 hour post sahur and 1-2 hour pre iftar : To detect subclinical hypoglycemia
• 2 hour post iftar, dinner : To detect subclinical hyperglycemia
WHEN TO BREAK FASTING :
• If blood glucose < 3.3 mmol/L at any time of day
• If blood glucose < 3.9 mmol/L during first few hours of sahur
• If blood glucose > 16.7 mmol/L, check ketones in urine
• Avoid fasting on sick days
THINGS THAT INVALIDATE FASTING :
• Transfusion of blood
• Receiving via a needle nourishing substances. With regard to injections which do not replace food and drink, rather they are administered for the purpose of medical treatment – such as penicillin or insulin or for the purpose of vaccinations, these do not affect the fast, whether they are intravenous or intramuscular. But to be on the safe side, these injections may be given at night.
• Kidney dialysis
• Donating blood but if a person suffers a nosebleed, his fast is valid because that happened involuntarily.
• Vomiting deliberately
• Menstruation
THINGS THAT DO NOT INVALIDATE FASTING :
• Enemas, eyedrops, eardrops, tooth extraction and treatment of injuries.
• Medical tablets that are placed under the tongue to treat angina but avoid swallowing any residue.
• Insertion of anything into the vagina such as pessarie or a speculum or the doctor’s fingers for the purpose of medical examination
• Insertion of medical instruments or IUD into uterus.
• Anything that enters the urinary tract of a male or female such as a catheter tube or medical scopes or opaque dyes inserted for the purpose of x-rays or medicine or a solution to wash the bladder.
• Fillings, extractions or cleaning of teeth so long as avoiding swallowing anything that reaches the throat.
• Rinsing the mouth, gargling, sprays etc. so long as avoiding swallowing anything that reaches the throat.
• Oxygen or anaesthetic gases as long as that do not give the patient any kind of nourishment.
• Anything that may enter the body via absorption through the skin such as creams, ointments etc.
• Insertion of a fine tube via the veins for diagnostic imaging or treatment of the veins of the heart or any part of the body.
• Taking samples from the liver or any other part of the body so long as that is not accompanied by administration of solutions.
• Endoscopy so long as that is not accompanied by administration of solutions or other substances.
• Introduction of any medical instruments or materials to the brain or spinal column.
REFERENCES :
- Diabetes and Ramadan: Practical Guidelines International Diabetes Federation (IDF), in collaboration with the Diabetes and Ramadan (DAR) International Alliance April 2016
- Al-Arouj M, Assaad-Khalil S, Buse J, et al. Recommendations for management of diabetes during Ramadan: update 2010; Diabetes Care. 2010; 33(8): 1895-902.
- Mafauzy M. Repaglinide versus glibenclamide treatment of Type 2 diabetes during Ramadan fasting. Diabetes Res Clin Pract. 2002; 58(1): 45-53.
- Glimepiride in Ramadan (GLIRA) Study Group. The efficacy and safety of glimepiride in the management of type 2 diabetes in Muslim patients during Ramadan. Diabetes Care. 2005; 28(2): 421-422.
- Al Sifri S, Basiounny A, Echtay A, et al. The incidence of hypoglycaemia in Muslim patients with type 2 diabetes treated with sitagliptin or a sulphonylurea during Ramadan: a randomised trial. Int J Clin Pract. 2011; 65(11): 1132-1140.
Dr. M Saifuddin
MBBS (DMC, K-56)
FCPS (Medicine), MD (Endocrinology)
FACE (USA), FACP (USA)
Assistant professor (Endocrinology)
Dhaka Medical College
Platform Academic Division / Ariful Islam Neloy