
বাইরে বের হবার আগে আয়নায় নিজেকে দেখে কিছুটা খটকা লাগলো সুরঞ্জনার। খুব ভালো করে লক্ষ্য করার পর মুখের দুইপাশে কেমন অসামঞ্জস্যতা মনে হলো তার, যেন বাম পাশের চোয়ালের পেছন দিকটা একটু ফুলে উঠেছে। জীবনানন্দের সঙ্গে পাড়ার কফি শপে দেখা করতে গিয়ে তিনিও দেখলেন সুরঞ্জনার মুখে আজ যেন বিষণ্নতার ছায়া, কিছু একটা অস্বাভাবিক তারও মনে হলো।
পরদিন সকালে ঘুম থেকে উঠে আয়নার সামনে গিয়ে এবার বেশ ভয় পেয়ে গেলো সে, ফুলে যাওয়া অংশটি ধীরে ধীরে বড় হচ্ছে এমন মনে হলো তার। ডেন্টালে পড়ুয়া কাছের এক বান্ধবীকে জানানোর পর একজন ম্যাক্সিলোফেসিয়াল সার্জনের চেম্বারের ঠিকানা দিল সে। অতঃপর আজ সন্ধ্যায়ই শহরের নামী দামী ম্যাক্সিলোফেসিয়াল সার্জন ডা. পলাশের চেম্বারে উপস্থিত হলো সে।
ডা. পলাশের চেম্বারে সেসময় বিডিএস তৃতীয় বর্ষে অধ্যয়নরত এক ছাত্র তুষারের আগমন ঘটে। সুরঞ্জনা চেম্বারে ঢুকে ডা. পলাশকে সব জানালে ডিটেইল্স হিস্ট্রি ও এক্সামিনেশন করার পর তাকে একটি ওপিজি এক্সরে করবার পরামর্শ দেন এবং কাল রিপোর্টসহ আবারো দেখা করতে বলেন। সুরঞ্জনা চলে যাবার পর ডা. পলাশের কাছে ছাত্রের প্রশ্ন-
-স্যার আপনি রোগীর যাবতীয় হিস্ট্রি শুনে কি সন্দেহ করছেন? যদি একটু বলতেন।
– তুষার, সুরঞ্জনার যাবতীয় হিস্ট্রি শুনে ও ইন্ট্রা ও এক্সট্রা ওরাল এক্সামিনেশন করার পর
আমার বেশ কিছু রোগ নিয়েই সন্দেহ হচ্ছে যার মধ্যে একটি হলো অ্যামেলোব্লাস্টোমা।
– স্যার অ্যামেলোব্লাস্টোমার সম্পর্কে আমি জানতে আগ্রহী। আপনার কাছে এ ব্যাপারে বিস্তারিত জানতে চাচ্ছিলাম।
– ঠিক আছে তবে, মনযোগ দিয়ে শোনো।
মানুষের মুখের অভ্যন্তরে odontogenic এবং non odontogenic নানান ধরনের tumour হতে পারে ।Ameloblastoma হচ্ছে odontogenic tumour গুলোর মধ্যে অন্যতম। ইতিহাস পর্যালোচনা করলে দেখা যায়-
🟣 ১৮২৭ সালে সর্বপ্রথম Cuzack এর দ্বারা স্বীকৃত হয় এটি।
🟣এরপর ১৮৭৯ সালে Falksson এটিকে follicular cystoid tumor হিসেবে ব্যাখ্যা দেন।
🟣 পরবর্তীতে ১৯৩৪ সালে সর্বপ্রথম Ivy এবং Churchill ” ameloblastoma” টার্মটি ব্যবহার করেন।
এক কথায় বলতে গেলে, ameloblastomas are benign epithelial neoplasms in which the epithelium contains ameloblasts like cells and stellate reticulum like cells, indicating its odontogenic nature. ১৯৯২ সালে দেয়া বিশ্ব স্বাস্থ্য সংস্থার এক সংজ্ঞানুযায়ী- Ameloblastoma
Is a benign, but locally invasive epithelial odontogenic neoplasm, with strong tendency to recur.
-ধন্যবাদ স্যার, এখন মিস সুরঞ্জনার হিস্ট্রি শুনে আপনার ameloblastoma সন্দেহ করার কারণটা যদি একটু বলতেন। সেই সাথে সামগ্রিকভাবে Clinical feature গুলো কেমন হতে পারে ?
– ঠিকাছে আমি একসাথে বুঝিয়ে বলছি।
👉 Firstly, ameloblastoma is the most common type and the most common neoplasm in the jaws.
👉Secondly, these are usually first recognized between ages of 30 and 50 years and are rare in children and old people. মিস সুরঞ্জনার বয়সের সঙ্গে যে বৈশিষ্ট্য কিনা সামঞ্জস্যপূর্ণ ছিল।
👉Thirdly, 80% of ameloblastomas form in the mandible and of these 75% develop in the posterior molar region and often involve the ramus. যা কিনা সুরঞ্জনার swelling টি এক্সামিনেশন করবার সময় আমার চোখে পড়ে।

👉Fourthly, It is usually symptomless untill the swelling is noticed. It can grow to enormous size and cause major disfigurement. সুরঞ্জনার দেয়া হিস্ট্রি অনুযায়ী হঠাৎ করে তার বাম চোয়ালের পেছন দিকে ফুলে যাওয়া ছাড়া তেমন কোনো complain ছিলনা। এজন্যই আমি এটা সন্দেহ করি। এবার বুঝলে ??
– জ্বি স্যার। বুঝতে পেরেছি। That means, the typical presentation of ameloblastoma is a rounded, bony swelling of the posterior alveolar bone, body and angle of the mandible. এমন কি ?
-হ্যাঁ তুমি ঠিক বলেছো। এর সাথে আরো মনে রাখতে পারো in typical presentation there is no ulceration, which would be a feature only seen in very large tumours that have perforated the cortex.
– ধন্যবাদ স্যার। আমি একটি জিনিস লক্ষ্য করেছি আপনি যখন ameloblastoma নিয়ে বলছিলেন তখন plural form ব্যাবহার করেছেন। তার মানে কি এটার বিভিন্ন প্রকারভেদ রয়েছে ?
– Yes, there are several types of ameloblastoma. According to the clinical classification, There are:
💁 Unicystic ameloblastoma
💁 Conventional or multicystic or solid ameloblastoma
💁Peripheral (extraosseous) ameloblastoma
💁 Malignant ameloblastoma
💁 Pituitary ameloblastoma (craniopharyngioma or Rathke’s pouch
tumour)
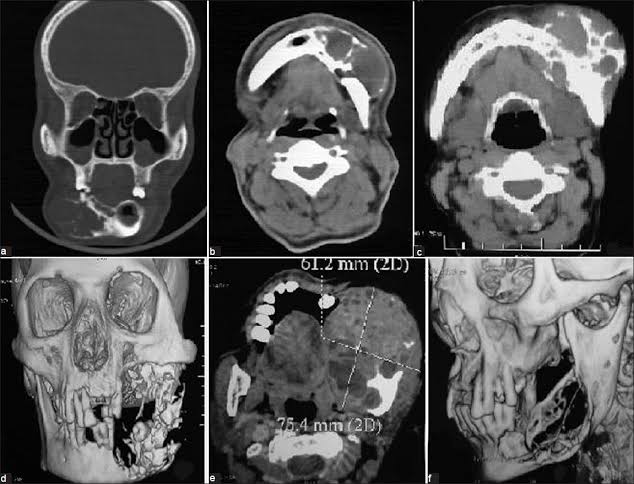
-Thank you so much sir. এখন, আমার আরেকটি প্রশ্ন হলো কাল মিস সুরঞ্জনার OPG (orthopentamogram ) রিপোর্টে কি কি সুনির্দিষ্ট বিষয়ে দেখে আমরা নিশ্চিত হতে পারি এটিই ameloblastoma?
– Okay I’m explaining.
🟢Radiographically, ameloblastomas typically form rounded, cyst like, radiolucent areas with well defined margins. আকারে ছোটো ameloblastoma সাধারণত unilocular হয়ে থাকে। অন্যদিকে আকারে বড় ameloblastoma এর ক্ষেত্রে ‘ soap bubble ‘ অর্থাৎ সাবানের ফেনার মত কিংবা ‘honeycomb’ অর্থাৎ মৌমাছির চাকের মত multi locularity দেখা যেতে পারে। এছাড়াও ameloblastomaর একটি অতি গুরুত্বপূর্ণ বৈশিষ্ট্য হলো এর bucco lingual expansion.
– স্যার, ameloblastomaর মত multilocular radiolucency আমরা কি আর কোনো ক্ষেত্রে দেখতে পারি?
– খুবই ভালো প্রশ্ন। হ্যাঁ আরো কিছু ক্ষেত্রে এমন দেখতে পারি যেমন-
odontogenic keratocyst,
giant cell granuloma,
odontogenic myxoma প্রভৃতি। তবে শুধু radiological feature জানলেই হবেনা। কেননা ameloblastoma পুরোপুরি কনফার্ম করতে আমাদের দরকার biopsy। যার জন্য histopathology জানাও একইরকম গুরুত্বপূর্ণ। আমি এ বিষয়ে তোমাকে বিস্তারিত বলছি-
Histologically two patterns are mainly seen. They are:
🟡Follicular
🟡Plexiform
Besides, there are other histological subtypes. For example:
🛑Acanthomatous
🛑Granular cell type
🛑 Desmoplastic type
🛑Mural type etc.
💥In the plexiform type, there are thin, interlacing strands of epithelium, but typical ameloblast are often not seen in this pattern.
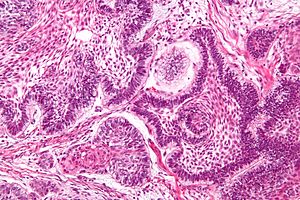
💥On the other hand, the follicular type of ameloblastoma(which is the most common) shows islands with an outer layer of tall, columnar, ameloblast- like cells
with reversed polarity surrounding a core of loosely arranged polyhedral or angular cells, resembling stellate reticulum.
(Also cyst formation is common and cysts can be as large as a few centimetres in diameter.)
-বুঝতে পেরেছি স্যার। এখন জানতে চাচ্ছি, অ্যামেলোব্লাস্টোমার ট্রিটমেন্টের ক্ষেত্রে তাহলে মূলত কি কি করা যেতে পারে?
বলছি, শোনো।
🎯– পূর্বে ameloblastomaর ট্রিটমেন্টের ক্ষেত্রে ব্যাপকভাবে ব্যবহৃত হতো curettage. তবে এতে করে recurrence rate বেড়ে যাওয়ায় এখন আর এটি প্রচলিত নয়।
🎯Now, ameloblastomas are best treated by resection of the lesion with a
marginal clearance of 1.5-2 cm of normal bone to prevent recurrence.
🎯The lesion may be resected as block resection with or without
continuity defect based on the integrity of inferior cortex.
🎯 Radiologically a minimum of 1 cm residual mandible inferior cortex is
required postoperatively to prevent pathologic fracture.
🎯Inferior alveolar nerve should be sacrificed if it lies within the lesion.
🎯Therefore, radical excision is
essential, preferably maxillectomy.
🎯 Peripheral ameloblastomas are treated by excision, as usually there is no alveolar bone involvement.
🎯If prior biopsy indicates involvement of bone, block resection with continuity defect is the choice of treatment.

-অসংখ্য ধন্যবাদ স্যার। এর আগে কখনো বিস্তারিতভাবে বিষয়গুলো বোঝার সুযোগ হয়নি। আপনার কারণে আজ তা সম্ভব হলো।
-তৃতীয় বর্ষের ছাত্র হবার পরেও তোমার জানবার আগ্রহ দেখে আমি সত্যই অভিভূত এবং ধন্যবাদ ধৈর্য্য ধরে আমার কথাগুলো শোনার জন্য। চূড়ান্ত বর্ষে গিয়ে এ সম্পর্কে আরো ভালো জানতে পারবে বলে আশা করি।
এই বলে ডা. পলাশ বাইরে অপেক্ষারত পরের রোগীকে রুমে প্রবেশ করতে বললেন। আর তুষার সালাম দিয়ে ডা. পলাশের চেম্বার থেকে সেদিনের মত বিদায় নিল।
Ref: Cawson’s Essentials of Oral Pathology and Oral Medicine (9th Edition)
Textbook of Oral and Maxillofacial Surgery – S.M Balaji
লেখা: হৃদিতা রোশনী
শহীদ সোহরাওয়ার্দী মেডিকেল কলেজ, ডেন্টাল ইউনিট
সেশন (২০১৫-১৬)