
Stein Leventhal first described it in 1935.
It is the commonest endocrine disorder in women of reproductive age.
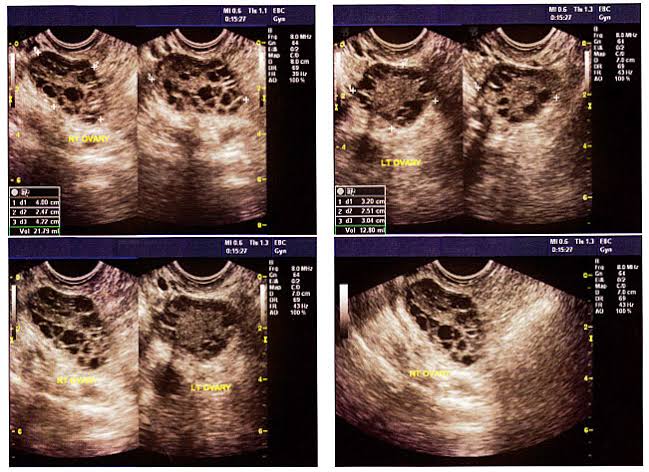
This disorder is associated with excessive androgen production and impaired ovarian follicular growth leading to anovulation.
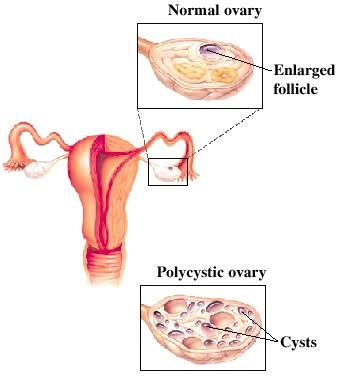
Fig : Polycystic ovarian syndrome.
SYMPTOMS:
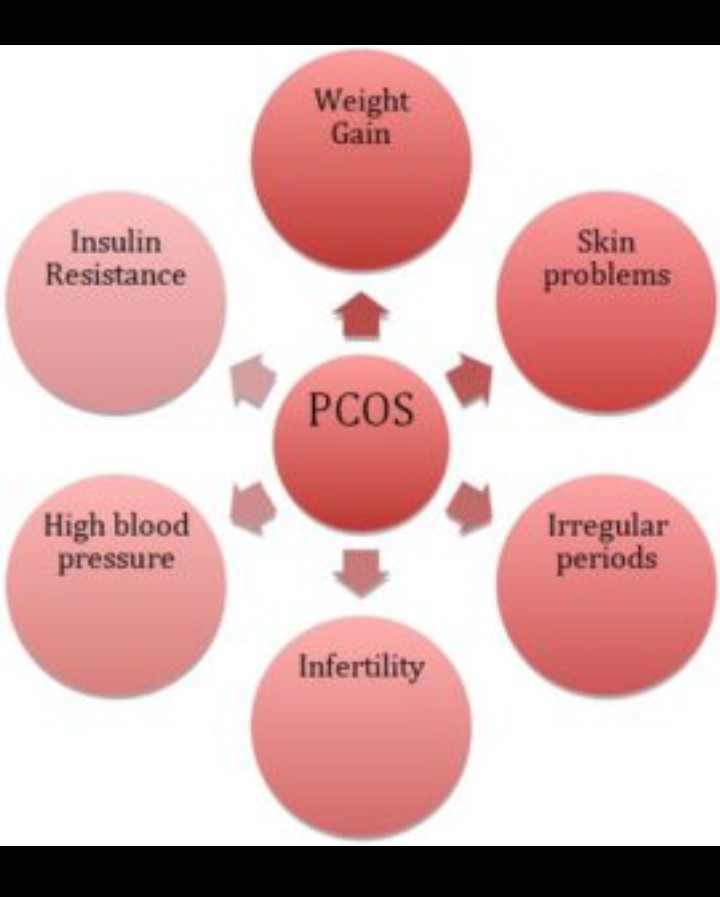
➡ Irregular periods or no periods at all (Oligomenorrhoea, Amenorrhoea)
➡ Weight gain
➡ Excessive hair growth (Hirsutism)
➡ Thinning hair / hair growth
➡ Acne, Oily skin
➡ Infertility (Because of irregular ovulation / anovulation)
➡ Dark patches on skin (Acanthosis nigricans, skin thickened and pigmentation)
HAIR-AN Syndrome:
HA = Hyperthyroidism
IR = Insulin resistance
AN = Acanthosis Nigricans
PATHOLOGY:
Macroscopic findings –
1. Ovaries are enlarged.
2. Stroma is increased.
3. The capsule is white and pearly white in color.
4. On section multiple follicular cysts are found.
Microscopic findings –
1. Thickened tunica albugina.
2. The cysts are follicles, at varying stages of maturation and atresia.
3. Theca cells hypertrophy.
PATHOPHYSIOLOGY:
1. Systemic endocrine dysfunction
2. Disorientation of intrafollicular environment for proper follicular maturation.
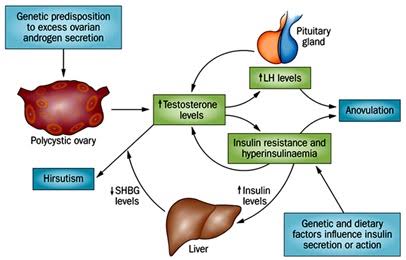
⚫Systemic endocrine dysfunction:
Excess androgen production.
➡ Defective ovarian steroidogensis Androstenedione is not converted to estradiol due to aromatase enzyme deficiency.
Stimulation of theca cells by high LH and by insulin like growth factor-q (IGF-1)
➡ Hyper-adrenalism
Excess androgen is produced by stress, Hyperprolactinemia, P450 C17 enzyme hyper function.
➡ Hyperinsulinemia
➡ Hyperprolactinemia
⚫Disorientation of intrafollicular environment:
➡ Low FSH level follicular growth is arrested at different phases of maturation.
➡ Excess androgen is produced from theca cells of ovary.
➡ Anovulation is usual due to defective follicular growth, maturation and absence of LH surge.
Endocrine abnormalities in PCOS:
1. Elevated androgen
2. Elevated LH
3. Low FSH
4. Elevated Estrogen
5. Elevated Insulin
6. Elevated prolactin
7. Hypothyroidism
⚫Long term consequences:
1. Endometrial hyperplasia and carcinoma.
2. Risk of developing diabetes mellitus.
3. Risk of HTN and CVD due to abnormal lipid profile.
How PCOS affects your body:
⚫Infertility:
Normal pregnancy এর ovulation এর জন্য LH serge এবং mature follicle প্রয়োজন হয়। কিন্তু PCOS এ LH serge ছাড়াই LH বেড়ে যায় এবং FSH কমে যায়। তাই Mature follicle তৈরি হতে পারে না।
এভাবেই ovulation এ ব্যাঘাত ঘটে এবং Infertility হয়।
⚫Irregular period:
নিয়মিত মাসিক হওয়ার জন্য Uterine shedding হওয়া প্রয়োজন। কিন্তু PCOS এ ovulation হয় না বলে Uterine shedding হতে পারে না। যার কারণে Irregular periods হয়।
⚫Metabolic disorder:
PCOS এবং obesity উভয়ই High blood pressure, high blood sugar, high lipid এর সম্ভাবনা বাড়িয়ে দেয়। এই কারণগুলো পরবর্তীতে Metabolic disorder করে Heart disease, stroke আর diabetes এর ঝুঁকি বাড়িয়ে দেয়।
⚫Sleep Apnea:
Obesity এর কারণে অনেকে নিদ্রাহীনতায় ভোগে। অন্যান্যদের তুলনায় PCOS আক্রান্ত obese মহিলারা ৫-১০ গুন বেশি ঝুঁকিতে থাকেন।
Note: আরো অনেক কারণে sleep Apnea হতে পারে।
⚫Endometrial Carcinoma:
Ovulation stage এ uterine shedding হয়। যদি প্রতিমাসে ovulation না হয় পরবর্তীতে তা Endometrial Carcinoma তে পরিণত হতে পারে।
⚫Depression:
Hormonal changes এবং symptoms যেমন অনাকাঙ্ক্ষিত চুলের বৃদ্ধি মহিলাদের অনুভূতিতে নেতিবাচক প্রভাব ফেলে যার কারণে সে depression এবং anxiety তে ভোগে।

⚫Differential Diagnosis:
1. Hyperprolactinemia
2. Late onset adrenal neoplasm
3. Hypothyroidism
4. Cushing’s syndrome
5. Ovarian and adrenal neoplasm
How to Diagnose PCOS:
A>> History taking
B>> Physical examination –
1. Vital Signs
2. Weight
3. If any problem then breast examination.
4. per abdominal examination.
5. Per vaginal examination – Bilateral enlarged ovaries
C>> Investigation
1. FSH, LH
2. Serum prolactin
3. Serum TSH
4. Serum creatinine
5. Serum Testosterone, Progesterone
6. Blood sugar
7. Fasting lipid profile
8. USG of L/A or pelvic organ, if married also can do TVS.
NOTE: Don’t advice those tests at a time (because too much cost effective)
Treatment:
1) Metformin (OD/ BD/ TDS)
2) OCP (For menstrual regularity)
3) Clomiphene Citrate (Period Day 2-6) for 6 cycle (Infertility for ovulation)
Advice:
১. রক্তে শর্করার পরিমাণ বেশি থাকলে নিয়ন্ত্রণ করুন ( PCOS-এর কারণে রক্তে শর্করার পরিমাণ বাড়ার সম্ভাবনা রয়েছে)।
2. ওজন হ্রাস করুন।
৩. নিয়মিত অনুশীলন, হাঁটাচলা করুন।
৪. অ্যালকোহল সেবন করা, ধূমপান পরিহার করুন।
৫. স্বাস্থ্যকর খাবার গ্রহণ করুন এবং তৈলাক্ত-চর্বিযুক্ত খাবার এড়িয়ে চলুন।
৬. চিন্তামুক্ত থাকুন।
৭.হৃদরোগে আক্রান্ত ব্যক্তি এসকল নিয়ম মেনে চলুন।
Dr. Tania Hafiz
2003-2004
Z.H Sikder Women’s Medical College and Hospital
কারিতাস ঠিকানা প্রকল্প
মিরপুর, রুপনগর, ঢাকা-১২১৬,কারিতাস বাংলাদেশ
⚫প্ল্যাটফর্ম একাডেমিক / সাদিয়া কবির ⚫