
এটা একটা cardiac emergency condition যেখানে pain হবে stable angina / classical angina এর মতোই কিন্তু কোনভাবেই rest, minimal exertion বা GTN দেওয়ার পরেও দূর হবে না। Acute coronary syndrome এ দুটি cardiac condition আছেঃ
– Unstable Angina
– Myocardial infarction
একজন patient আসলো এবং সে history দিবে, family history of cardiac disease বা তা যদি না থাকে তাহলে সে একাধিক modifiable risk factor এর history দিবে।
আমার cardiology এর এক শ্রদ্ধেয় স্যার বলেন,
“Symptom and history is a big thing of coronary artery disease.”
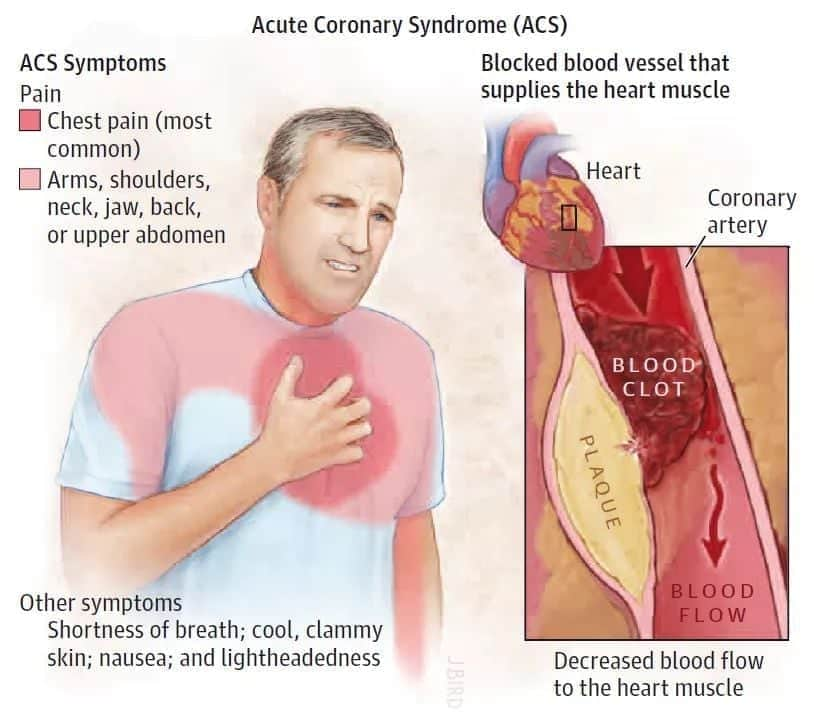
Acute coronary syndrome (Unstable angina, MI) তে সাধারণত Atherosclerosis বা other form of disease এ যে plaque form করে সেগুলোর dynamic obstruction হয় এবং পরে এইগুলা coronary artery (Right & Left) তে partial বা complete occlusion করে দেয়। তাহলে হচ্ছে কি?
– Myocardium এ blood supply কমে যায়, তার জন্য পরে হচ্ছে ischemia। এই consequences এর জন্য তৈরি হয় lactic acid। আর এই lactic acid গুলো nerve fibre কে irritation করে এবং এর জন্য হয় pain। তাহলে clinical feature হবেঃ
- Central chest pain, radiate to jaw, neck, shoulder etc.
- Breathlessness.
- Collapse/ syncope.
✴ Signs of sympathetic activation:
– Pallor
– Sweating
– Tachycardia
✴ Signs of vagal activation:
– Bradycardia
– Vomiting
✴ Signs of myocardial dysfunction:
– Hypotension
– Cold periphery
– Narrow pulse pressure
– Oliguria
– Quick first Heart sound
– Third Heart Sound
– Signs of complication
✴ Mitral regurgitation
✴ Pericarditis
এখন কথা হচ্ছে, এই যে Acute coronary syndrome এর দুটি component: Unstable Angina আর Myocardial infarction এগুলো আমরা আলাদা করবো কিভাবে?
আসুন দেখা যাকঃ
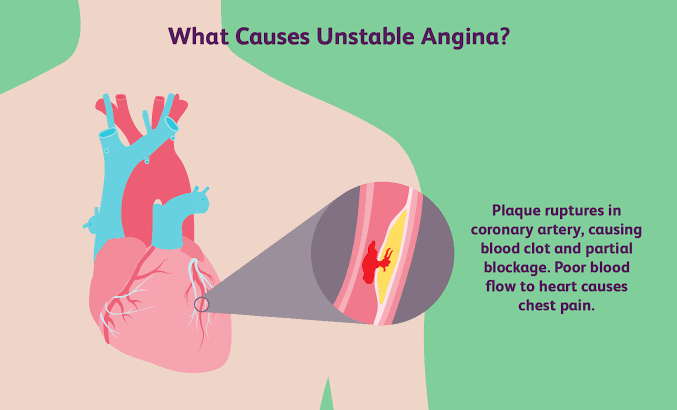
◼ Unstable angina: এটা হয়ে থাকে Atherosclerosis বা others cause এ যে plaque ফরমেশন হয় সেইটার ulceration বা rupture হয়ে যায় মানে আপনি যদি definition বিবেচনা করেন তাহলেঃ It may be defined as angina of new onset or rapidly worsening of angina which is not removed by rest, minimal exertion or GTN.
➡ Investigation of Unstable Angina :
– 12 Lead ECG: ST depression
T inversion
– Cardiac enzyme: normal or no detectable rise যেখানে Myocardial infarction এ highly rise পাওয়া যাবে।
➡ Management:
– Hospitalization – Complete bed rest, oxygen inhalation
– Sedatives যদি দরকার হয় – Anti anginal drugs:
✔ Beta blockers,
✔ Calcium channel blocker,
✔ GTN
– Low molecular weight Heparin (Enoxaparin, Tinzaparin, Raviparin) for 5 to 7 days.
✴ যদি সবগুলো failure হয় তাহলে coronary Angiogram for revascularization।
✴ আর patient কে advice দিতে হবে smoking, alcohol ইত্যাদি বন্ধ করে দিতে।
Exercise এর limitation আনতে হবে।
◼ Myocardial infarction:
প্রথমেই আসি Heart এর blood supply এ। Heart কে মূলত supply দেয় Right and left coronary artery যেগুলো arise হয় Aortic root থেকে। Left coronary artery আবার দুই ভাগে হয়ঃ LAD (Left Anterior descending artery) আর CX (circumflex) artery।
LAD supply দেয় anterior surface of Left Ventricle এবং anterior aspect of interventricular septum। আবার circumflex artery supply দেয় lateral wall আর inferoposterior segment of Left Ventricle এ।
এবার আসুন Right Coronary artery তে। RCA সাপ্লাই দেয় SA node, AV node, Right ventricle আর পরে continuation হয় PDA ( posterior descending artery)। এটা supply দেয় posterior segment, inferior segment of Left ventricle এ।
✴ LAD: Pumping capacity
✴ LCA: Pain
✴ RCA: Arrhythmia
এটা অনেকটা suspect করা হয়। LAD occlude হলে বা RCA occlude হলে যে pain হবে না ব্যাপারটা এমন নয়৷ এগুলো occlusion হলেও pain হয় বা Arrhythmia হয়।
এখন আসুন ECG লিডেঃ
- Anterior surface: V1 to V6
- Inferior surface: Lead 2, 3, aVF
- High lateral surface: Lead 1, aVL
- Lateral surface: V5, V6, Lead 1, aVL.
- Anterolateral surface/ Extensive anterior: V1 to V6, lead 1, aVL.
- Posterior MI: V1 and V2.
Heart এর posterior surface এর জন্য কোন লিড নেই। আবার কিছু additional lead ব্যবহার করা হয় যারা হচ্ছে V3R, V4R যেগুলো পরে নাম হয়ে যায় V3, V4। এটা দিয়ে diagnosis করা হয় Right ventricular infarction and associated with inferior infarction।
আবার এই posterior infarction এ ECG তে ST depression এবং Tall R wave, T wave wide, Tall, upright থাকবে। এটা আমরা পাব Lead V1, V2 তে। যেহেতু posterior part কে সাপ্লাই দিচ্ছে CX এর কিছু portion এবং PDA এর কিছু portion। কিন্তু আমরা যদি Heart এর dominance বিবেচনা করি তাহলে 60% হচ্ছে Right dominance মানে হিসাবে RCA occlusion হচ্ছে।
Inferior MI এর বেলায়ও প্রায় একই ঘটনা। এখানে আমরা ST elevation, pathological Q wave, T inversion পাব Lead 2, 3, aVF এ।
আবার আরেকটি কথা এখানে bradycardia পাওয়া যাবে vagal activation এর জন্য।
আবার আরেকটি hypothesis দাড় করানো যায়। যদি inferior MI এ Right coronary artery occlude হয় তাহলে SA node এর ফাংশন কিছুটা depressed হয়ে যায় কারণ RCA 60% সাপ্লাই দেয় SA node এ। এই activity depress হওয়ার জন্য হয়ে থাকে junctional rhythm। এই nodal/ junctional rhythm এর জন্য sinus bradycardia হয়।
এজন্য Inferior MI এর খুব important complication গুলো হচ্ছেঃ
– Sinus bradycardia
– Junctional rhythm
– Heart block
– RV infarction
Anterior MI: এখানে ECG চেঞ্জ হয় V1 to V6 এ। সাধারণত এখানে LAD / LCA occlude হয়ে যায়৷
High Lateral MI: ওই একই lead 1, aVL এ চেঞ্জ হয়। CX artery occlusion হয়ে যায়।
Anterolateral MI: এখানে চেঞ্জ হয় lead 1, aVL, V1 to V6.
High lateral: Lead 1, aVL
Lateral MI: Lead 1, aVL, V5, V6
Septal MI: Lead V2 to V4
Subendocardial MI: Symmetrical T wave inversion in all chest lead.
✴ Cardiac biomarkers: সাধারণত Acute myocardial infarction এ এই enzyme / biomarker গুলোর high rise থাকে যেখানে unstable angina তে থাকেই না বললেই চলে। এই biomarker গুলোর মাঝেঃ
✔ Troponin I and T: এটা অন্য গুলোর চেয়ে specific। কারণ তারা normal কন্ডিশন এ absent থাকে এবং cardiac myocytes ইনজুরির পর তারা blood এ appear হয়। এরা rise হয় 2 to 4 hour, Highest pick up: 12 to 15 hours এবং normal এ ফিরে আসে 7 days এ।
এছাড়া কিছু কিছু condition আছে যেখানে MI হয়নি কিন্তু serum Troponin বেড়ে গেছে-
– Cardiac surgery
– Catheter ablation
– Prolonged hypotension
– Sepsis
– End stage renal disease (ESRD)
– Stroke
– Acute pulmonary edema
– Pulmonary embolism etc.
✔ CPK MB: এরা blood এ appear হওয়া শুরু করে 4 to 6 hours, highest হয় 12 hours এবং normal হয় 2 to 3 days এ।
✔ AST (Aspartate aminotransferase): এরা appear হওয়া শুরু করে 12 hours, highest হয় 24 hours এবং normal হয় 3 to 4 days এ।
✔LDH (Lactate dehydrogenase): এরা appear হয় 12 hours, highest হয় 72 hours আর normal অবস্থায় ফিরে আসে 7 to 10 days এ।
N.B: এই Time duration গুলো কিছু কিছু বই vary করতে পারে।
✴ CBC (Complete blood count): Neutrophilic leukocytosis
✴ Inflammatory marker: CRP rise
ESR rise.
✴ Radiography: Chest X ray
কারণ হচ্ছে কোন pulmonary edema বা আগেকার Heart disease থেকে cardiomegaly হয়েছে কিনা তা দেখার জন্য।
✴ Echocardiography: এই Echocardiogram করা হয় Ventricular function assessment এর জন্য complication detection (mural thrombus, cardiac rupture, septum rupture, mitral regurgitation, pericardial effusion) করার জন্য।
✴ Coronary Angiogram: এটা হচ্ছে Myocardial infarction এর diagnosis করার জন্য সবচাইতে reliable method। আর হবেই বা না কেন? কারণ এই Angiography, artery এর anatomical information, nature of CAD এবং কোন জায়গায় occlude হয়েছে তা নিয়ে ধারণা দেয়। এই coronary angiogram এর কিছু indication রয়েছে। যেমনঃ
- ST segment elevated MI
- High risk of non ST segment elevated ACS
- Recurrent/ severe angina unresponsive to medical treatment.
- Positive exercise test following MI
- Cardiac Arrhythmia when clinical suspicion of CAD
- Pre operatively advanced age (50 yrs) patient who required valve surgery
- When PCI or CABG is being considered.
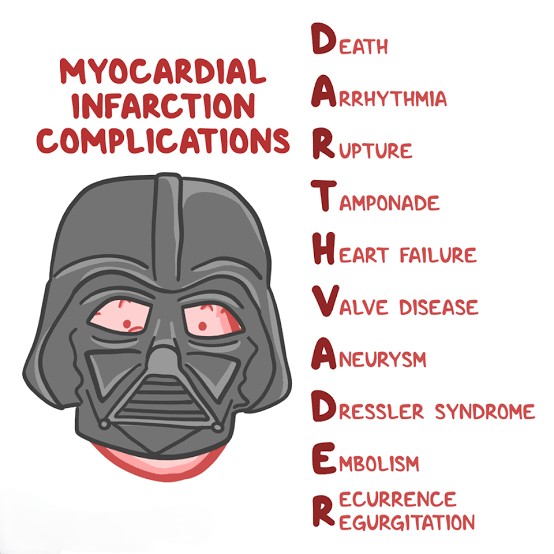
এবার আসুন complication এ। একে আমরা দুইভাগে ভাগ করব। Early complication আর late complication।
চলুন early complication এ –
1. VPC/ PVC (Premature ventricular contraction): ধরা যায় এখান থেকেই সব arrythmia হয়ে থাকে। যেমন :
- Ventricular fibrillation,
- Ventricular tachycardia,
- Accelerated idioventricular rhythm,
- Atrial tachycardia,
- Atrial fibrillation,
- Atrioventricular block,
- Sinus tachycardia,
- Sinus bradycardia,
- RV infarction,
- Heart block (common in inferior MI)
2. Acute pericarditis
3. Cardiac tamponade
4. Cardiogenic shock
5. Biventricular Heart failure
6. Rupture of interventricular septum leading to Ventricular septal defect (VSD): তাহলে হয়ে থাকে left to right shunt এবং যেটা পরে Heart failure এর prognosis অনেক বাড়িয়ে দেয়।
এর Diagnosis করা হয় doppler echocardiography এবং Right Heart catheterization দিয়ে। আর treatment হিসাবে surgical repair করা হয়।
7. Rupture of papillary muscle and chordae tendineae: এই কন্ডিশন এ একজন patient present করে –
- Dyspnoea,
- Pulmonary edema,
- Shock এবং
- Mitral regurgitation নিয়ে৷
তাহলে examination এ আমরা pansystolic murmur, third heart sound পাবো এবং confirm করা যায় echocardiography দিয়ে।
✔ Explanation :
এবার 2 to 5 number point এর complication গুলো দেখুন। এটার consequences গুলোকে এমন ভাবে সাজানো যায় : Myocardial infarction > Pericarditis > Exudative accumulate into pericardial space > Pericardial effusion and cardiac tamponade > Ultimately Heart failure.
এবার আসুন late complication এ :
1. Ventricular remodeling: Heart এর একটা segment এ MI হল। তারপরে কি হয়? Non infarcted segment এ হয় hypertrophy আর infarcted segment এ হয় thinning। তারপর ওই thinning segment এর workload বেড়ে যায় এবং complication হিসাবে ventricular remodeling হয়৷ এটার আরেকটা explanation বিবেচনা করলে :
- Abnormal myocardial metabolism
- Myocyte apoptosis
- Regulation of gene expression.
আমরা এই remodeling prevent করার জন্য ACE inhibitor drugs দিয়ে থাকি।
2. Ventricular aneurysm: এটাও MI এর একটা late complication (10% patient)। সাধারণত বেশি হয়ে থাকে যদি কোন infarct related artery occlude হয়ে যায়। Diagnosis করা হয় echocardiogram দিয়ে। আর complication হিসাবে –
- Mural thrombus,
- Heart failure,
- Arrhythmia ডেভেলপ করে।
Treatment :
যদি Heart failure হয় তাহলে :
- Digoxin,
- ACE inhibitor,
- Beta blocker etc
Arrhythmia হলে Anti arrhythmic drug।
Thrombus বা embolus ফরমেশন হলে Anticoagulant drugs।
3. Dressler syndrome: একে post myocardial infarction ও বলা হয়। এটি হচ্ছে late complication যেটা হয়ে থাকে 2 to 10 week, MI এর পর। কারণ কি? MI এর পর myocardium এ necrosis হয়। আর এই necrosis myocardium এর বিপরীতে antibody production হওয়া শুরু করে (Anti myocardial antibody) যার জন্য হয় Ag-Ab reaction আর clinical feature হয় –
- Pain
- Pyrexia
- Pleurisy
- Pneumonitis
- Pericarditis / Pericardial effusion
Management of Dressler syndrome: High dose Aspirin 600 to 900 mg every 4 to 6 hourly,
Corticosteroid if severe,
If Chance of thromboembolism: Anticoagulant.
✴ Overall management of MI :
- Admitted in CCU
- Complete bed rest and oxygen inhalation (2 to 4 L/ minute)
- Morphine sulphate (5 to 10 mg)/ Diamorphine 2.5 to 5 mg with Metoclopramide.
- PCI / PTCI এটা হচ্ছে treatment of choice.
- কোন patient যদি 12 hours এর মাঝে আসে তাহলে PCI করা হয়৷ কিন্তু এটা 24 hour এ consider করা হয়৷ এটা খুব ভাল একটা procedure কারণ এতে coronary artery patency, left ventricular functional status সব maintain এ থাকে এবং Heart failure এর progress হয় না বললেই চলে।
✴ Other reperfusion therapy:
✔ Thrombolytic therapy: এটা করা হয়ে থাকে Streptokinase দিয়ে যদি কেউ 6 to 12 hours এর মাঝে আসে কিন্তু সবচাইতে বেশি ভালো হয় 2 hours এর মাঝে। এর কিছু indication আর contraindication আছে যা আমরা সবাই জানি।
এছাড়া Tenecteplase নামে আরও একটি ড্রাগ ব্যবহার করা হচ্ছে। এর বাজারমুল্য 67000 tk।
✔ Antithrombic therapy: বলা হয়ে থাকে 25% mortatily কমে যায় যদি oral Aspirin (300 mg) তাড়াতাড়ি দেওয়া যায়৷ এর সাথে P2Y12 antagonist (Clopidogrel, Ticagrelor) add করা হয়৷ আবার যদি aspirin এর intolarence থাকে তাহলে Clopidogrel 300 mg দেওয়া হয়।
✔ Low molecular weight heparin (S/C Enoxaparin 1mg/ kg body weight) বা S/ C Pentasaccharides (Fondaparinux 2.5 mg) দেওয়া যেতে পারে।
✔ Others: Sublingual GTN (300 to 500 micro gram, Beta blocker (Bolus I/ V atenolol 5 to 10 mg over 5 minute)। কিন্তু যদি contraindication থাকে তাহলে Verapamil, diltiazem দেওয়া যেতে পারে।
✔ ACE inhibitor (Enalapril 10 mg twice daily) যদি tolerance না হয় তাহলে ARB (Valsartan 40 to 160 mg daily) বা Aldosterone receptor antagonist (Spironolactone 25 to 50 mg বা Eplerenone 25 to 50 mg daily)
✔ Lipid lowering agent: Atorvastatin 80 mg daily.
✔ এবং সাথে advice যেমন smoking cessation, diet control, Hypertension and diabetes control, regular exercise।
✴ আর যদি সব measure ফেইল হয় তাহলে ICD (Implantable Cardioverter defibrillator device).
➡ Primary prevention: যাদের high risk of arrhythmic death রয়েছে যেমন –
- Myocardial infarction and left ventricular ejection fraction < 30%
- Cardiomyopathy
- Long QT syndrome.
➡ Secondary prevention: যাদের MI এর evidence আছে যেমনঃ
– Survivors of ventricular fibrillation and
– Pulseless VT etc.
MD. Mehedi Hasan
Session: 2015-16
Kyamch, Sirajgonj
প্ল্যাটফর্ম একাডেমিক/ দিলোয়ারা ইয়াসমিন প্রিয়া