
"ANTEPARTUM HEMORRHAGE"★Definition:
Bleeding from or into the genital tract after the 28th week of pregnancy but before the birth of the baby.
***(NB: >12- <28 th weeks bleeding: Abortion.
<12 weeks bleeding: Abortion/ Ectopic/ Molar pregnency)
★Causes:
- Placental (70%):
– Placenta previa (35%)
– Abruptio placenta (35%) - Extra placental (5%):
– Cervical polyp
– Carcinoma cervix
– Vericose vein
– Local trauma - Unexplained (25%)
এখন আলোচনা করব “Placenta Previa” সম্পর্কে।
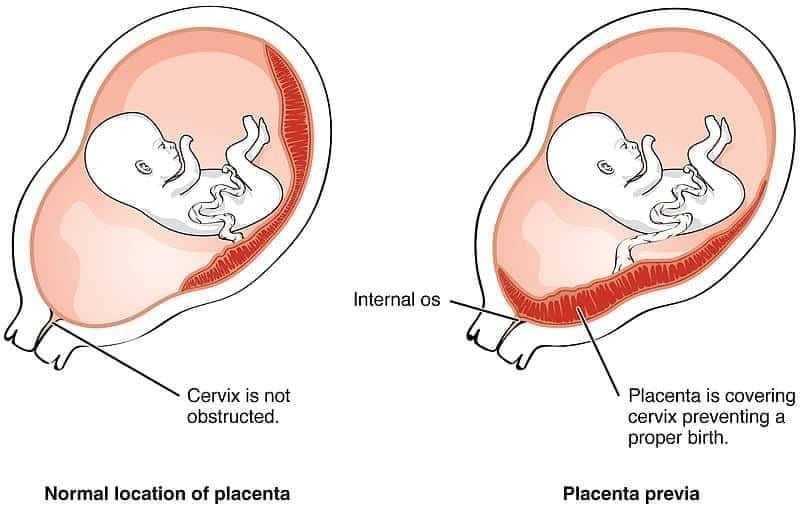
"PLACENTA PREVIA"★Definition:
When the placenta is implanted partially or completely over the lower uterine segment.
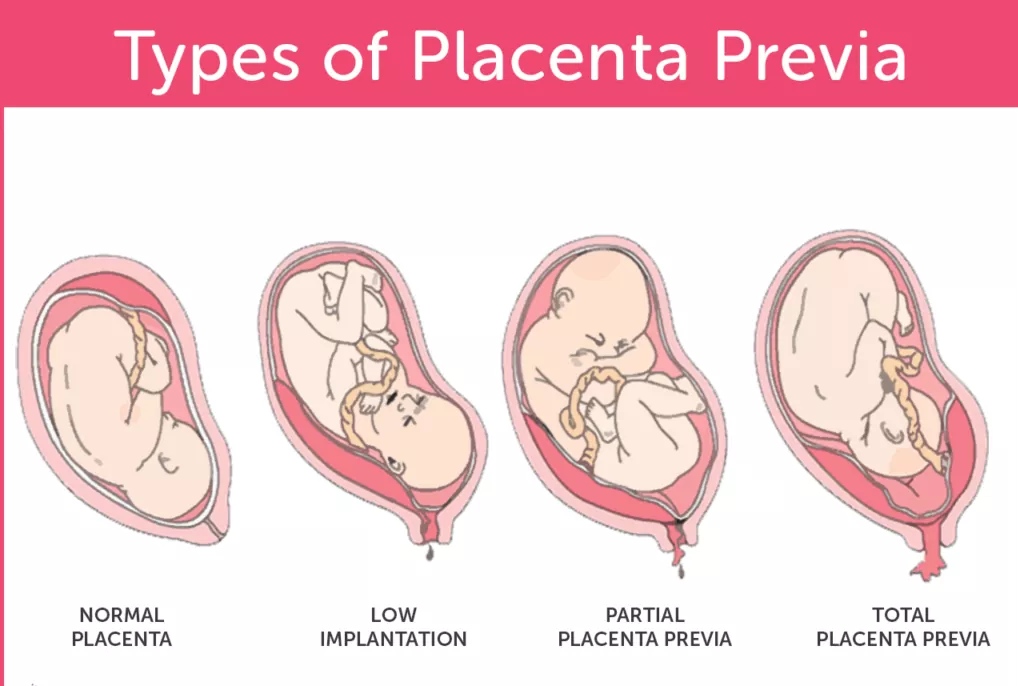
★Types:
•Type— I (Low- lying): The major part of the placenta is attached to the upper segment and only the lower margin encroaches into the lower segment but not up to the os.
•Type— II (Marginal): The placenta reaches the margin of the internal os but does not cover it.
•Type— III (Incomplete or partial central): The placenta covers the internal os partially (covers the internal os when closed but does not entirely do so when fully dilated).
•Type— IV (Central or total): The placenta completely covers the internal os even after it is fully dilated.
★Degree
•Mild- Type- l,
Type- ll(anterior)
•Major- Type- ll (posterior),
Type- lll &
Type- Iv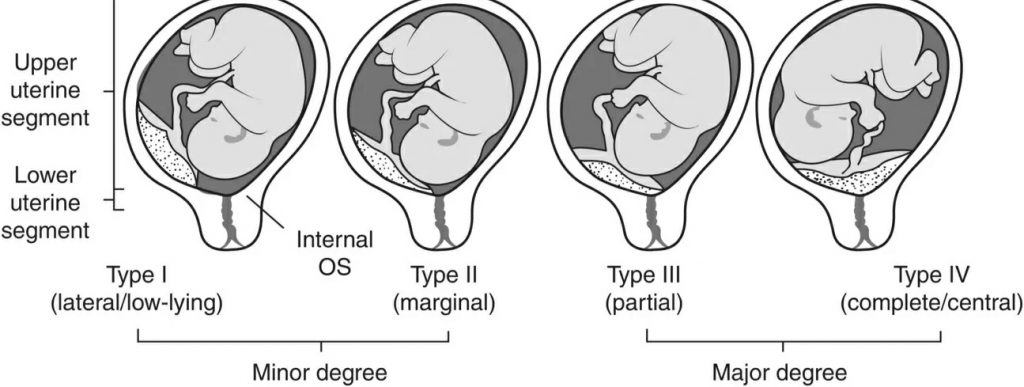
★Causes of bleeding:
Disproportionate growth of lower segment of uterus and placenta.
★The mechanisms of spontaneous control of bleeding are:
– Thrombosis of the open sinuses
– Mechanical pressure by presenting
parts
– Placental infraction
★★C/F:
•Symptom:
– PVB which is sudden onset, painless and recurrent.
•Signs:
- General:
General condition and anemia are proportionate to the visible blood loss.
- Abdominal:
•The size of the uterus is
proportionate to the period of
gestation.
•The uterus feels relaxed,
soft, elastic and non tender.
•Persistence of
malpresentation.
•The head is floating.
•Fetal heart sound is present.
- Pelvic:
PV isn't done, only
inspection.•On inspection, continue bledding which is bright red in color.
★Investigation:
- CBC (Complete Blood Count)
- ABO, Rh grouping
- USG (Ultrasonography)
- MRI (Magnetic Resonance Imaging)
- Color dopler★★Mx:
★Immediate attention:
- Amount of the blood loss — by noting the general condition, pallor, pulse rate and blood pressure.
- Blood samples are taken for group, cross matching and estimation of hemoglobin.
- A large- bore IV cannula is sited and an infusion of normal saline is started and compatible cross matched blood transfusion should be arranged.
- Gentle abdominal palpation to ascertain any uterine tenderness and auscultation to note the fetal heart rate.
- Inspection of the vulva to note the presence of any active bleeding.
★Expectant Mx:
- Bed rest
- Periodic inspection
- Supplementary of hematinics
- Use of tocolytics, MgSO4 (if
associated with uterine contracrion)
- Anti D for Rh(-)
- Cervical cerclage may be
done(NB: <34 weeks: Steroid therapy is given)
•Then, continue of pregnancy upto 37 weeks of pregnancy.
★Active Mx:
•Vaginal delivery:
- When placenta edge is 2-3 cm away from internal cervical OS.
- When placenta edge is within 2 cm from internal cervical OS.(NB: Central placental previa is absolute indication for C/S)
★★★Complication:
★Maternal:
*During pregnancy:
- APH with varying degrees
of shock
- Malpresentation
- Premature labor
*During labor:
- Early rupture of
membrane
- Cord prolapse
- Intrapartum hemorrhage
*During puerperium:
- Sepsis
- Subinvolution
- Embolism
★Fetal:
- LBW (Low Birth Weight)
- Asphyxia
- IUFD (Intrauterine Fetal Death)
- Birth injuries
- Congenital malformationআজ এখানেই শেষ করছি।
INDRANIL JANA
Session: (2015-16)
Gazi Medical College, Khulna
প্ল্যাটফর্ম একাডেমিক/ সুমাইয়া আকবর লিরা
Pingback: Let’s talk about Antepartum Haemorrhage (Part-2) – Platform | CME